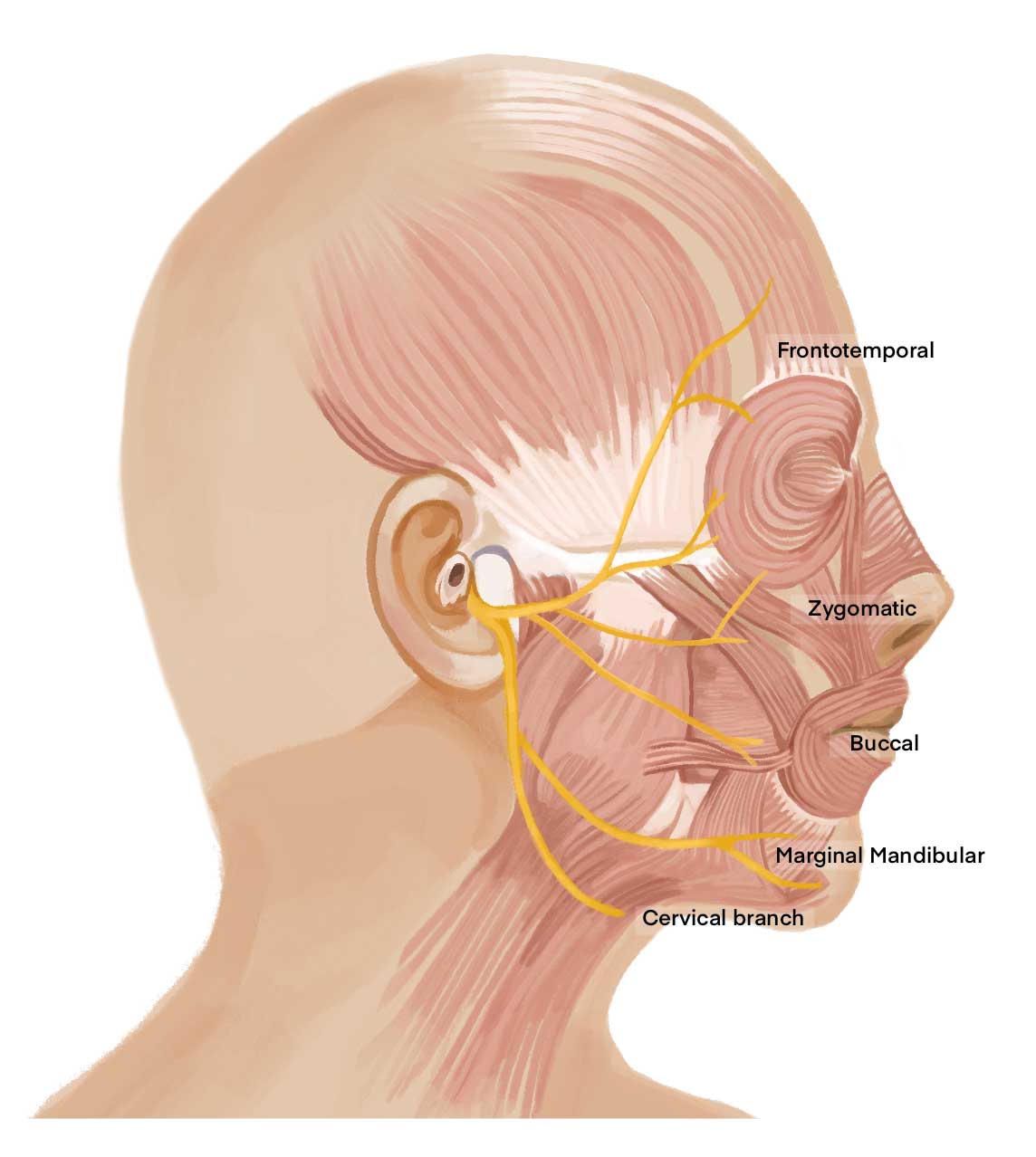
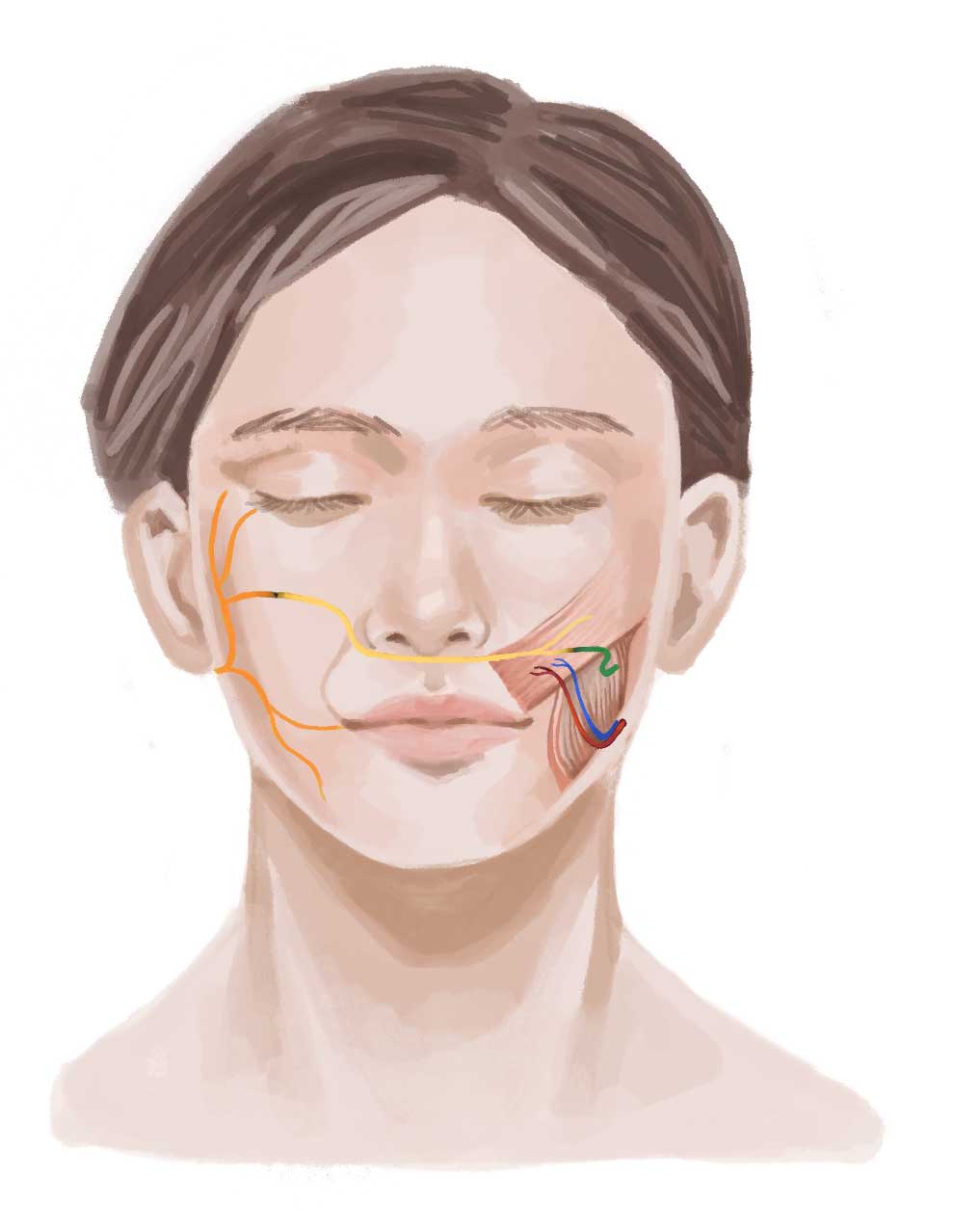
The facial nerve is the 7th cranial nerve and is the one which controls movement of the muscles of the face. It is divided into five main branches. These are responsible for important facial functions such as lifting of the eyebrows, eye closure and smiling. Paralysis results in severe impairment of the function and appearance of the face. Patients have symptoms such as dry eyes, drooling and inability to smile. In addition, taste sensation to the front of the tongue and tear production can be affected.
We provide sub-specialized care to treat facial nerve conditions in adults and children. Dr Wong has undergone intensive fellowship training in this area. The field of facial paralysis is very wide and every patient’s condition is different. The treatment plan thus needs to be individualized to suit your specific needs.
The facial nerve originates in the brain and leaves the skull below the ear, passing through the parotid salivary gland as it divides into branches that enter the facial muscles.
Facial paralysis can thus occur for a variety of reasons when the nerve is injured or interrupted along its course. These include salivary gland tumors, brain tumors, trauma or infections. It can also occur in children due to congenital abnormal development of the facial nerve.
Bell’s palsy is the leading cause of facial paralysis. The nerve becomes inflamed and swollen within its tight canal. This can be associated with viral infection. Patients generally report being suddenly unable to move their face, with the development of symptoms over 48-72 hours. Diabetes and pregnancy increase the risk of developing Bell’s palsy.
Patients who experience sudden facial paralysis should go to the Accident & Emergency Department without delay. After excluding other potential causes, appropriate initial steps include high dose oral steroids and antiviral medication. Eye protection (with eye drops and taping at night) is important to prevent corneal ulceration.
Other causes of facial paralysis such as tumor, trauma and inner ear infection must be ruled out, hence an ENT (ear, nose, throat) doctor is usually involved in the early management. Hearing tests or magnetic resonance imaging scan (MRI scan) may need to be performed in certain patients.
Most people start to get better within 3 weeks of when their symptoms start, although it can take them up to 6 months for nerve regeneration to be complete. 85% of patients can expect to recover fully from Bell’s palsy. 15% of patients can suffer from synkinesis and partial facial weakness.
“Synkinesis” refers to involuntary co-contractions between facial muscle groups. For example, patients may notice that their eye spontaneously closes when they smile. They may also have sensations such as twitching, spasms and tightness around the eye or mouth. This often began in the recovery phase because of lack of separation of upper and lower face movement. For examples, patients may lift up their cheek muscle to close their eye, inadvertently contributing to disorganized or abnormal facial nerve regeneration.
Our rehabilitation program by dedicated therapists is divided into phases depending on the stage of muscle recovery. In early cases, we aim to gently individually exercise the upper (eye) and lower facial (smile) muscle groups while reducing the development of synkinesis. For established synkinesis, a neuromuscular retraining program comprising of stretches, strengthening, synkinesis inhibition and imagery exercises can result in significant improvement. There are helpful resources on the internet such as the Facial Palsy series produced by QVH (Queen Victoria Hospital, UK) which can reinforce what has been taught. Acupuncture is not contraindicated if the patient wishes to undergo it. In contrast, any form of electrical stimulation can be harmful as it contracts the muscles with excessive force. It is best avoided as patients subsequently develop muscle tics and spasms which are hard to treat.
Botulinum toxin (Botox) injection is an important adjunct to relax the face and weaken unwanted synkinetic movements. This in turn facilitates the process of specific muscle strengthening. Treatment may be every 4-6 months for the first 1-2 years and thereafter, the interval can be lengthened or even halted depending on the progress of neuromuscular retraining. The treatment is generally affordable. As it is a medical procedure, it may be possible to utilize insurance or Medisave. Surgical procedures such as myectomy (removal of synkinetic muscles), blepharoplasty, brow lift, reduction of synkinetic muscles and smile reconstruction can improve symmetry and appearance.
These are the other main causes of facial nerve paralysis. Acoustic neuroma is the most common type of brain tumor involved. It is a benign (non-cancerous) growth that occurs on the eight cranial nerve which lies adjacent to the facial nerve. The eight nerve carries hearing information and balance signals from the ear to the brain. Symptoms of an acoustic neuroma include hearing loss, tinnitus (perception of noise ringing in the ear) and vertigo (spinning sensation). A hearing test and MRI can establish the diagnosis and the tumor may require removal by a neurosurgeon.
The treatment approach to facial paralysis in tumor cases depends on the findings during the operation. A conservative approach is prudent if the surgeon who performs the tumor removal feels that the nerve was saved during the operation. Patients will require eye care and sometimes temporary surgical procedures on a case-by-case basis. If the nerve was cut during the operation or if the facial palsy does not begin to improve by 6 months, then a more active approach must be taken.
If one or more facial nerve segments need to be removed because of tumor, they can be reconstructed using nerve grafts harvested from other areas of the body. This can be done either in the immediate setting (at the same time as the removal of the tumor) or as early as possible (within 3-6 months is preferable).
The nerve grafts can be connected to the same side facial nerve, or if this is not available, to the healthy side facial nerve. The nerve to the masseter muscle (one of the muscles for chewing) is also commonly used to provide more axonal input. As nerves regenerate at a speed of 1mm/day, between 3-9 months may be required before the nerve reaches the muscle and is able to activate it again.
If more than 12-18 months has elapsed from the time of onset of complete paralysis, the facial muscles are likely to be atrophied. Recovery may not happen even if the nerves are reconnected. Replacement of muscle function using functional muscle transfer is the ideal solution to allow the patient to smile again.
A strip of fascia lata can be harvested from the thigh via a small incision. The fascia lata is a layer that covers the thigh muscles and is relatively strong. A piece of it can be used as a hammock to suspend the lip and angle of the mouth. Although it is a simple procedure that can be performed even under local anesthesia injections, the position of the lip is fixed in an overcorrected position. In other words, patients do not have a dynamic smile. In addition, the fascia lata stretches with time and recurrence of lip drooping can be expected. Tightening of the fascia lata can be repeated in a second operation.
Other techniques such as face lift cannot produce a smile. However they can help improve the soft tissue drooping that also occurs in facial palsy.
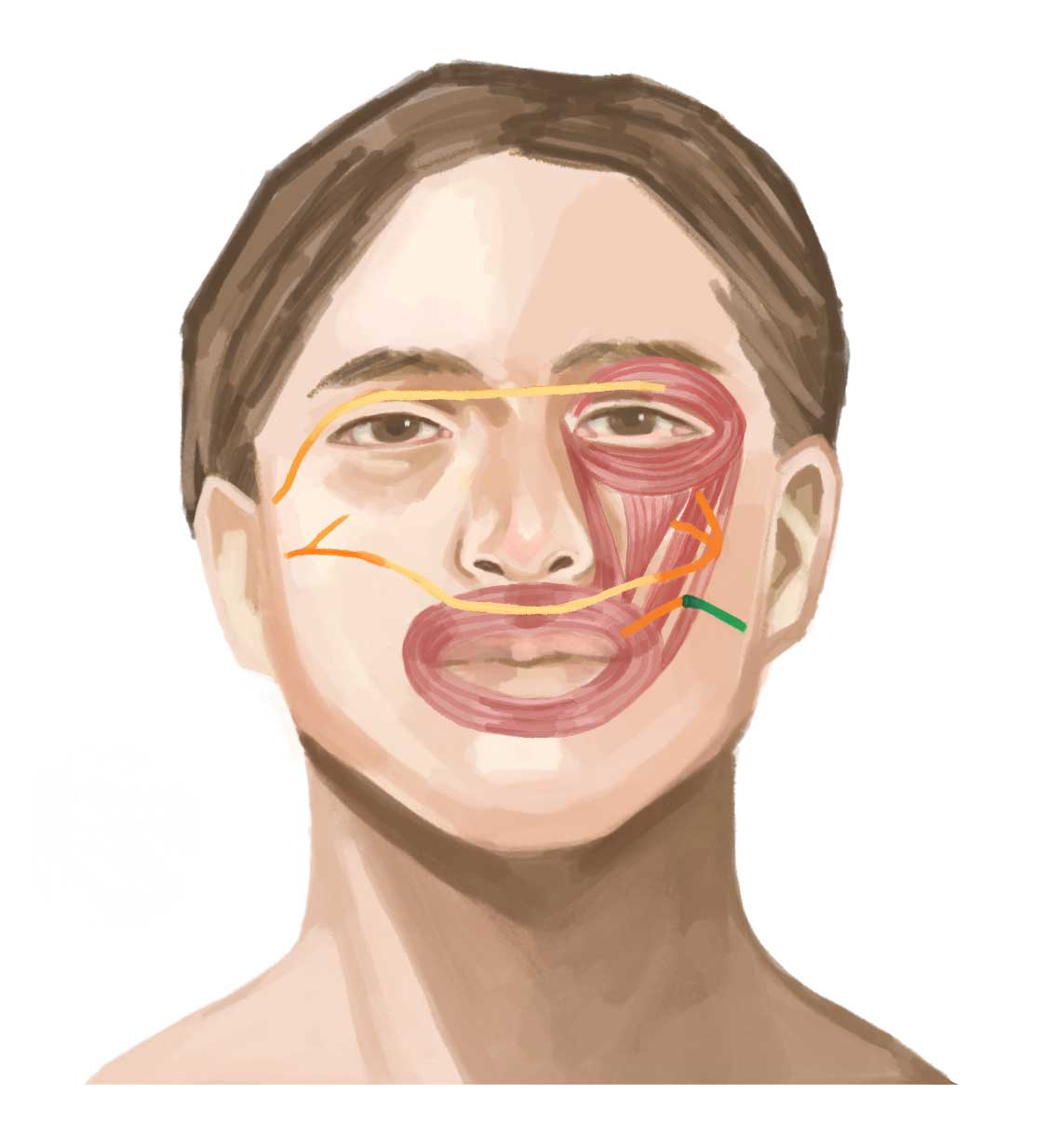
The temporalis muscle is one of the muscles responsible for jaw movement. One can locate it by feeling the temple area while biting down. This muscle can be diverted for smiling, by stitching its end to the smiling muscles around the mouth. A smile can be produced immediately post-operation by biting down. After going thru a post-operative rehabilitation program, a smile can be produced without conscious thought as early as few months after operation. Functional MRI has shown that the brain adapts by the process of cortical plasticity such that it recognizes the temporalis muscle as a “smiling muscle” instead of one for chewing.

When the facial muscles are in an atrophied state or are absent, muscle can be transferred from other parts of the body such as the back (Latissimus dorsi muscle) and thigh (Gracilis muscle) to replace them. After harvesting the muscle, there is no loss of function in the donor site as the body is designed with more than one muscle for the same job. The muscle is taken with its blood supply (artery and veins) and connected to blood vessels in the head and neck using microsurgery. Microsurgery is the joining of blood vessels under a microscope. The muscle is also harvested with its nerve which is connected to a branch of the healthy side facial nerve. After the nerve regenerates from the healthy side over a period 4-9 months, patients can smile as per normal without need for conscious activation.
There are 17 muscles of facial expression on each half of the face. Smiling is just one of the functions of the face. For example, restoration of brow position with brow lift techniques can reduce skin hooding and improve vision. This can be accomplished either by endoscopic techniques or by direct brow lift. A platinum weight can be placed in the upper eyelid to allow the eye to close easily. The lower eyelid can be tightened with techniques such as limited tarsorrhaphy, canthopexy, canthoplasty, inferior retractor recession or tendon sling. Facial asymmetry is also improved by minimally-invasive methods such as filler injection and fat grafting. Assessment by Dr Wong who specializes in facial nerve conditions is necessary to determine which techniques are most suitable in each individual case.
Exciting new advances include dynamic blink reanimation by functional muscle transfer, allowing patients to regain spontaneous eye closure.

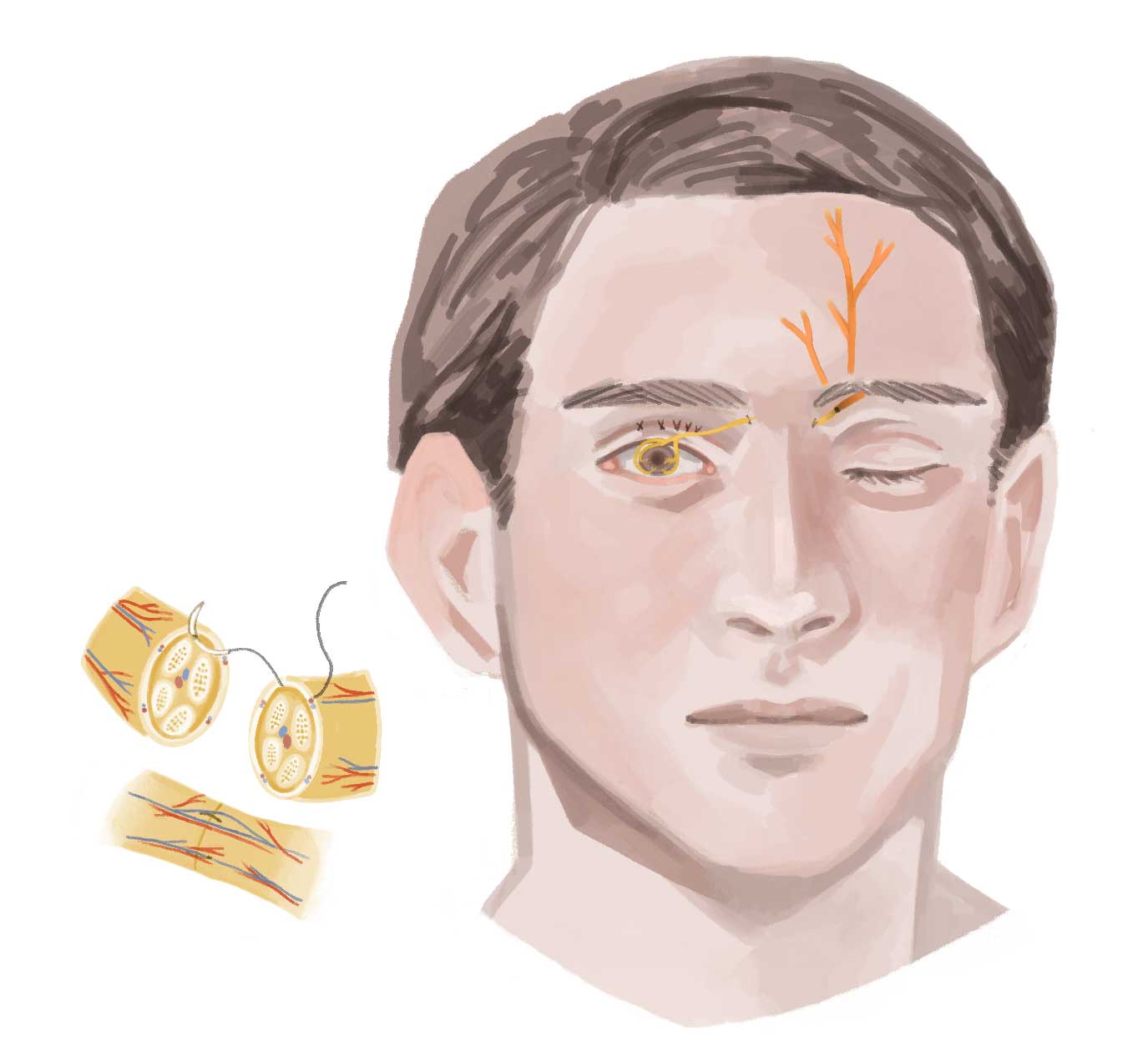
For patients with insensate corneas caused by concurrent 5th nerve palsy, corneal neurotization is becoming increasingly popular world-wide. This restores sensation to the cornea by using nerves supplying the forehead on the normal side. Patients can gain protective sensation to the eyeball surface and avoid going blind from unnoticed trauma.